Panic Attacks: Symptoms, Causes, Immediate Relief & Long-Term Treatment Options
Panic attacks are not dangerous — they are a misfired fight-or-flight response. Learn the symptoms, how to differentiate panic from a heart attack, evidence-based immediate relief techniques (box breathing, grounding, cold water, PMR), and long-term treatment with CBT.

In this article
A panic attack can arrive without warning: your heart races, your chest tightens, breathing becomes shallow, and a wave of overwhelming dread convinces you that something is catastrophically wrong. For many people, the first attack feels indistinguishable from a medical emergency. The experience is real — and the terror is completely understandable.
What is also true is this: panic attacks are not dangerous. They result from an overactivated stress-response system — one that has misfired and flooded your body with adrenaline in the absence of actual threat. Understanding precisely what is happening changes your relationship with it. Fear of the attack itself is one of the most powerful drivers of panic disorder. Knowledge interrupts that cycle.
Key Takeaways
You Don't Have to Navigate Panic Alone — Real-Time Support Is Available
Anxiety and panic can feel isolating and overwhelming. Dzeny provides private, structured AI-guided conversations that help you regulate emotions, understand triggers, and apply evidence-based coping tools anytime you need support.
Start Free Chat with DzenyWhat Is a Panic Attack?
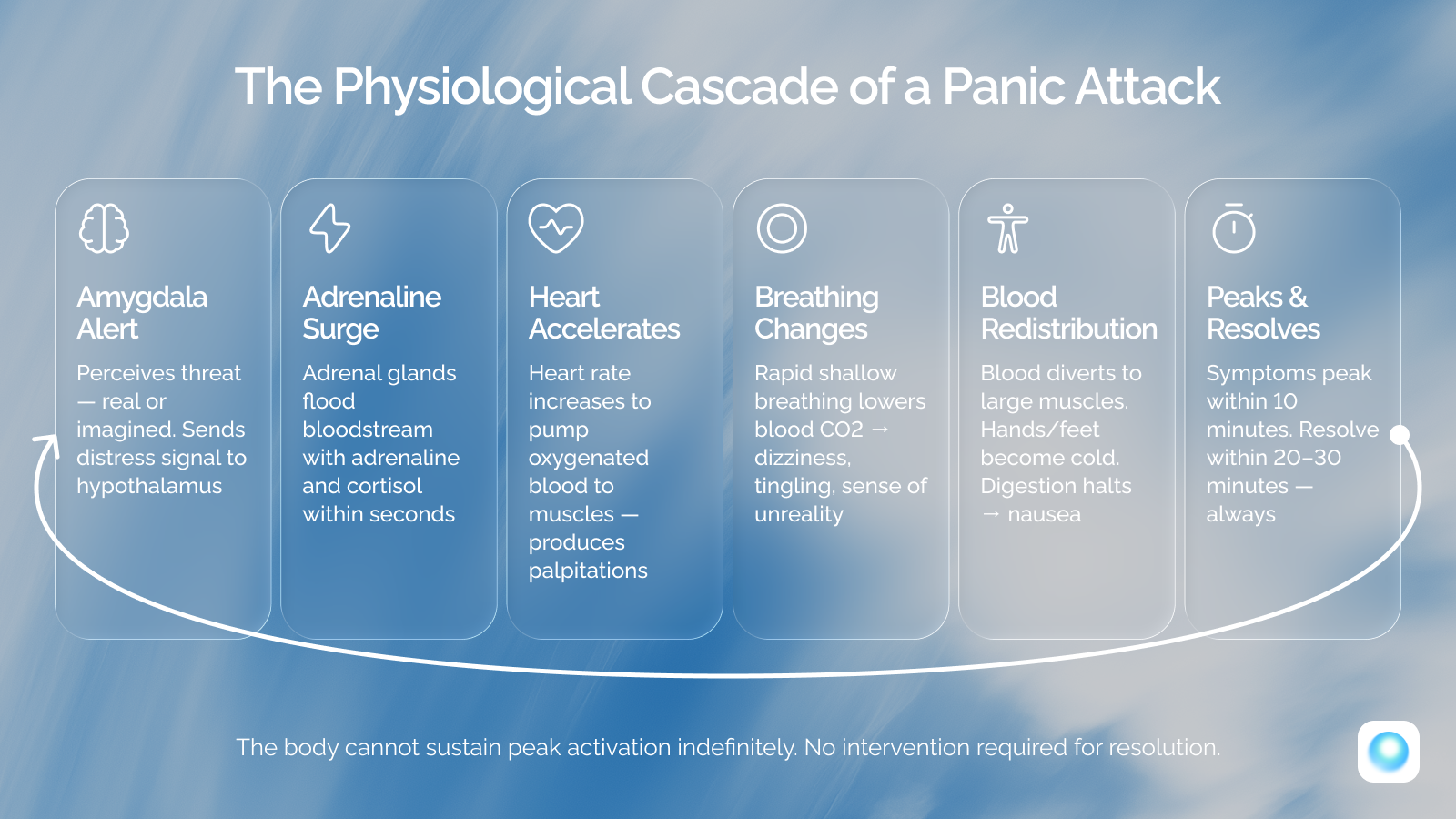
A panic attack is defined by the National Institute of Mental Health (NIMH) as a sudden episode of intense fear that triggers severe physical reactions when there is no real danger or apparent cause. During an attack, the amygdala — the brain's threat-detection center — interprets some internal or external signal as danger and immediately triggers the sympathetic nervous system. Stress hormones, primarily adrenaline, flood the bloodstream within seconds.
Most panic attacks peak in intensity within 10 minutes and resolve within 20 to 30 minutes. They are self-limiting — the body cannot sustain peak sympathetic activation indefinitely, and the response will subside regardless of whether you intervene. Understanding this timeline is itself therapeutic: in the middle of an attack, it feels as though the sensations will escalate without limit. They will not.
Physical Symptoms of a Panic Attack
The physical symptoms of a panic attack are among the most frightening aspects of the experience — precisely because they are so convincing. Chest pain that feels cardiac. Breathlessness that feels like suffocation. Dizziness that feels neurological. These are not imagined sensations. They are real, measurable physiological events produced by adrenaline surge, hyperventilation, and sympathetic nervous system activation.
According to the Cleveland Clinic, a panic attack is typically characterized by at least four of the following symptoms occurring simultaneously or in rapid succession:
| Physical Symptom | System | Physiological Mechanism |
|---|---|---|
| Rapid or pounding heartbeat | Cardiovascular | Adrenaline signals the heart to pump faster to deliver oxygenated blood to muscles |
| Chest pain or tightness | Musculoskeletal / Respiratory | Intercostal muscles tense; shallow breathing changes chest wall pressure |
| Shortness of breath | Respiratory | Rapid shallow breathing (hyperventilation) lowers blood CO2, creating sensation of air hunger |
| Dizziness and lightheadedness | Neurological / Vascular | CO2 drop and blood redistribution temporarily reduce cerebral perfusion |
| Numbness and tingling | Neurological | Hyperventilation-induced alkalosis affects peripheral nerve sensitivity |
| Sweating | Autonomic | Sympathetic activation triggers sweat glands to cool the body in preparation for exertion |
| Trembling and shaking | Musculoskeletal | Muscles primed for action maintain sustained micro-contractions; adrenaline causes visible shaking |
| Nausea and abdominal distress | Gastrointestinal | Blood diverted away from digestive system; gut's enteric nervous system responds to stress directly |
| Chills or hot flashes | Thermoregulatory | Blood redistribution leaves extremities cold; metabolic heat from activation creates flushing |
| Feeling faint | Vascular / Neurological | Vasovagal response in some individuals; CO2 imbalance affects cerebral blood flow regulation |
Expert Tip — When to seek medical evaluation
If you are experiencing chest pain, palpitations, or significant shortness of breath for the first time, always seek medical evaluation to rule out cardiac or respiratory causes before attributing symptoms to panic. A medical professional can confirm the diagnosis — and that confirmation itself reduces the fear that fuels future attacks.
Panic Attack vs. Heart Attack: A Critical Distinction
One of the most clinically important aspects of panic attacks is how convincingly they can mimic a cardiac event. The overlap in symptoms — chest pain, racing heart, shortness of breath, dizziness, a feeling of impending doom — is so significant that distinguishing between the two in the moment is genuinely difficult. Emergency medicine takes this overlap seriously.
The table below outlines the key differentiating features based on clinical guidance from the Mayo Clinic and Cleveland Clinic. These are patterns, not absolute rules. If you are uncertain, seek medical evaluation. Do not use this table to self-diagnose during an acute episode — if you are experiencing severe chest pain for the first time, particularly with radiation to the arm or jaw, call emergency services immediately.
| Panic Attack | Heart Attack |
|---|---|
| Sharp, localized chest pain; often described as pressure | Crushing pressure — "an elephant on the chest" |
| Pain rarely radiates — typically stays in the chest | Often radiates to left arm, jaw, neck, or back |
| Sudden onset, often at rest or without physical exertion | Often during/after physical exertion; can occur at rest |
| Peaks within minutes; resolves within 20–30 minutes | Sustained and progressive — does not resolve without treatment |
| Dizziness, tingling, derealization, fear of dying | Cold sweat, severe fatigue, jaw pain, nausea without dizziness |
| Symptoms reduce as nervous system calms | No meaningful relief — symptoms persist or worsen |
| Common in 20s–30s; no cardiovascular risk profile required | More common with age; associated with cardiac risk factors |
What Causes Panic Attacks?
One of the most disorienting aspects of panic attacks is that they can appear to arrive from nowhere. In reality, panic attacks always have causes — though those causes are not always obvious in the moment. They involve a combination of biological vulnerability, accumulated stress load, specific situational triggers, and learned patterns that the nervous system has developed over time.
Primary Risk Factors
Specific Triggers
When Panic Attacks Become Panic Disorder
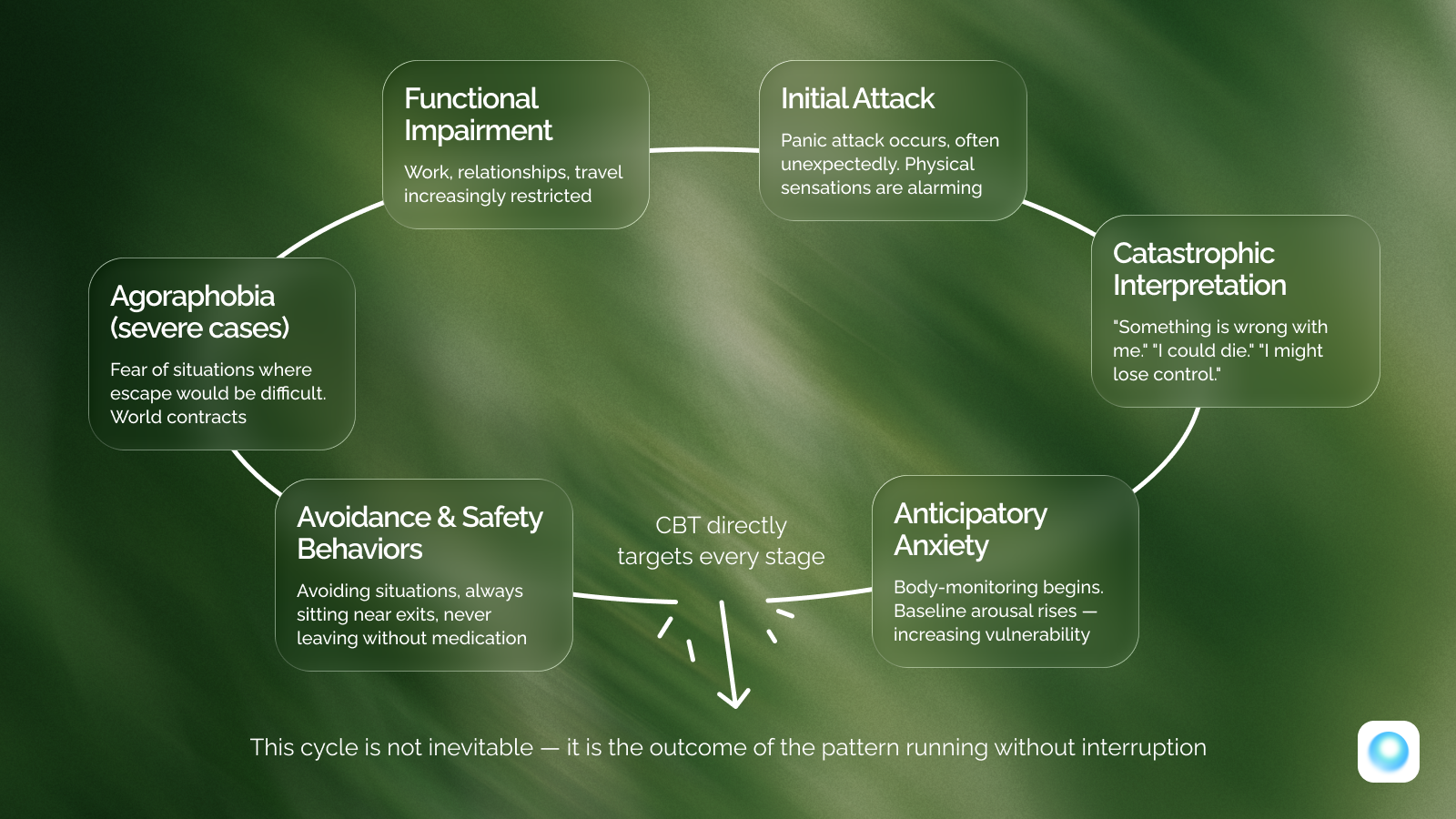
A single panic attack, or even several isolated attacks during an acutely stressful period, does not constitute panic disorder. According to NIMH, panic disorder is diagnosed when three conditions are met: recurrent unexpected panic attacks occur; at least one attack is followed by a month or more of persistent concern about future attacks; and the person makes significant behavioral changes to avoid future episodes. Approximately 2–3% of U.S. adults meet criteria in any given year.
The central feature that distinguishes panic disorder from isolated attacks is anticipatory anxiety — a chronic, low-grade state of dread about when the next attack will occur. Without treatment, the behavioral restrictions compound and the world gets smaller. In severe cases, agoraphobia can develop — a fear of situations where escape might be difficult or help unavailable if panic struck.
Evidence-Based Immediate Relief Techniques
Effective panic intervention works by targeting the nervous system directly — using physiological inputs that the autonomic nervous system responds to regardless of what you are thinking. The four techniques below are supported by clinical practice and recommended by major U.S. health institutions because they interrupt the stress response at the physiological level, not just the psychological one. Practice them when you are calm so they are accessible when you are not.
Technique 1: Box Breathing — Resetting the Stress Response
During a panic attack, rapid shallow breathing lowers CO2 levels, causing dizziness, tingling, and chest tightness. These sensations are produced by the breathing pattern itself. Box breathing restores blood gas balance and stimulates the parasympathetic nervous system through the vagus nerve. Slow exhalation, in particular, sends a direct signal to the brain that the threat has passed.
Box Breathing: Step-by-Step
Within 2–3 minutes of consistent practice, heart rate typically slows and mental clarity begins to return.
Technique 2: 5-4-3-2-1 Grounding — Interrupting Catastrophic Thinking
Panic attacks are fueled not only by physical sensations but by catastrophic interpretations: "I'm dying," "I'm losing control." The 5-4-3-2-1 method shifts attention to the actual sensory reality of the present moment — which is almost always objectively safe — by re-engaging the prefrontal cortex.
The 5-4-3-2-1 Grounding Method
Specificity matters: "I see a cracked tile near the window" is more effective than "I see a room."
Technique 3: Cold Water and the Dive Reflex
When cold water contacts the face or neck, the mammalian dive reflex initiates an immediate cardiovascular recalibration: heart rate slows, sympathetic activity reduces, and a brief physiological calm is produced. This technique is particularly useful when breathing exercises alone are insufficient. It requires no skill development and produces results within seconds.
Technique 4: Progressive Muscle Relaxation (PMR)
Panic causes muscles to tighten automatically. PMR exploits the contrast between deliberate muscular tension and release. Tense each muscle group firmly for 5 seconds, then release completely for 10 seconds — progressing from feet up through calves, thighs, abdomen, chest, arms, shoulders, and face. One full cycle takes 15–20 minutes and produces significant reduction in physiological arousal. Even 5 minutes targeting the most tense areas provides meaningful relief.
Struggling with Symptoms That Feel Scary or Uncontrollable?
Racing heart, chest tightness, dizziness — panic symptoms can feel overwhelming. Dzeny helps you process sensations calmly and guides you through breathing and grounding techniques in real time.
Talk About Your SymptomsLong-Term Treatment Options
Immediate techniques manage individual episodes; long-term treatment changes how frequently episodes occur and how much power they have over your life. According to NIMH and the Cleveland Clinic, panic disorder is highly treatable — the question is not whether treatment works, but which combination of approaches is right for your situation.
Cognitive Behavioral Therapy (CBT): First-Line Treatment
CBT is widely considered the most effective psychological treatment for panic disorder. According to the American Psychological Association, CBT demonstrates significant symptom reduction for panic disorder, with many patients achieving lasting improvement after a structured course of treatment — typically 12 to 20 sessions. CBT works by targeting three interconnected elements: distorted thinking patterns that interpret normal sensations as dangerous; physical sensitization to ordinary physiological changes; and avoidance behaviors that prevent the nervous system from learning the feared situations are actually safe.
Lifestyle Factors That Directly Affect Panic Frequency
The nervous system operates within a physiological context directly shaped by sleep quality, physical activity, and what you consume. Many people with panic disorder discover that targeted lifestyle changes reduce attack frequency significantly.
| Lifestyle Factor | Evidence and Practical Guidance |
|---|---|
| Sleep | Sleep deprivation increases amygdala reactivity by 30%+ (UC Berkeley research). Target 7–9 hours with a consistent schedule, cool dark room, and no screens 1 hour before bed. |
| Caffeine | Directly mimics fight-or-flight activation. For panic-prone individuals, consider limiting to under 200mg daily or eliminating entirely if attacks are frequent. |
| Alcohol | Produces rebound sympathetic activation as it metabolizes. Reducing or eliminating alcohol typically reduces panic frequency within weeks. |
| Exercise | 30 minutes of moderate aerobic activity 3–5 times per week reduces anxiety symptoms by 20–30%. Also provides controlled exposure to elevated heart rate — desensitizing the body to sensations that trigger panic. |
| Routine and structure | Predictability reduces uncertainty-based anxiety. Consistent morning routines, regular mealtimes, and predictable sleep times reduce the cognitive load that sensitizes the nervous system. |
| Social connection | Isolation amplifies anxiety and removes the co-regulatory benefit of calm human presence. Even one or two close relationships provide a biological buffer against stress. |
How to Support Someone During a Panic Attack
Supporting someone during a panic attack requires calm presence, emotional validation, and simple physiological co-regulation — not clinical expertise or problem-solving. According to NIMH, the body in a panic attack is operating as if under genuine threat. The person is not exaggerating or choosing their response. Your goal is not to fix the attack — it will resolve on its own. Your goal is to help their nervous system feel safe enough to begin the natural de-escalation.
What to Do
What to Avoid
When to Seek Professional Help
Panic disorder responds significantly better to early treatment than to the "wait and see" approach. The research from NIMH and the Cleveland Clinic is consistent: panic disorder is highly treatable, and early intervention improves outcomes. Any single indicator below is sufficient justification for seeking an evaluation.
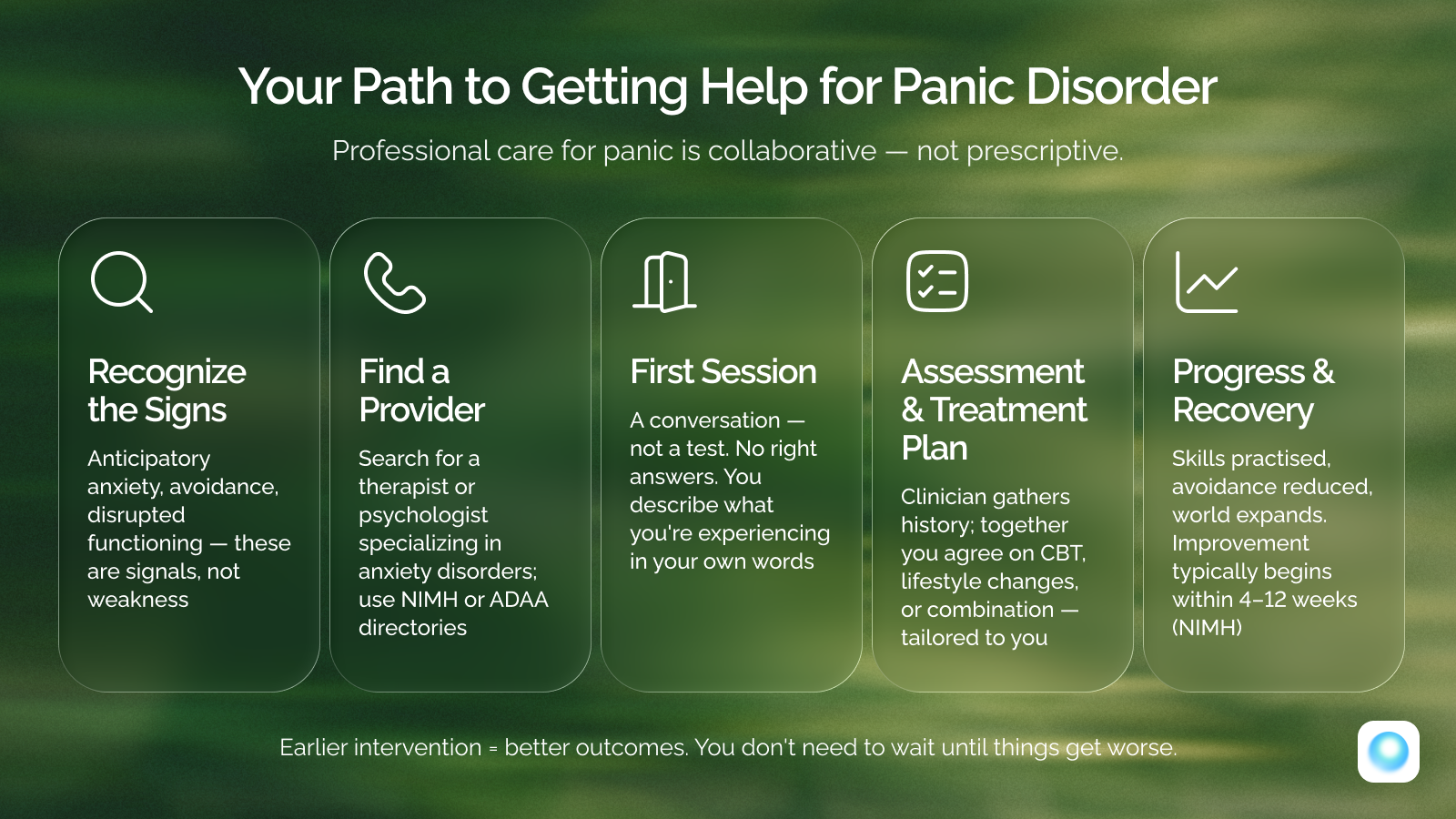
Seek Professional Help If
Seek immediate care
If you are having thoughts of self-harm or suicide, or experiencing chest pain for the first time with any cardiovascular risk factors — contact 988 (call or text) or go to the nearest emergency room.
Panic Is Powerful — But Treatable
Panic attacks can feel overwhelming and life-threatening, especially during early episodes. What the research makes consistently clear is that panic is not a condition you simply have to live with. It has a well-understood physiological basis, a well-documented set of maintaining factors, and a highly effective treatment approach in Cognitive Behavioral Therapy. Understanding the biology of panic reduces fear of the symptoms themselves. Immediate techniques interrupt episodes in real time. Long-term strategies — CBT, lifestyle modification, and professional support — significantly reduce frequency and severity and, for many people, produce lasting resolution.
Ready to Take Control of Panic Instead of Letting It Control You?
If panic attacks are affecting your daily life, AI-guided conversations can help you build coping skills, challenge catastrophic thoughts, and reduce fear — privately and at your own pace.
Begin Your JourneyReferences
- 1.NIMH. National Institute of Mental Health (NIMH) — Panic Disorder (2025)
- 2.Mayo Clinic. Mayo Clinic — Panic attacks: Symptoms & causes (2025)
- 3.Cleveland Clinic. Cleveland Clinic — Panic Attack & Panic Disorder (2025)
- 4.APA. American Psychological Association (APA) (2025)
- 5.988 Lifeline. 988 Suicide and Crisis Lifeline (2025)
- 6.APA. Journal of Consulting and Clinical Psychology (2025)
- 7.American Psychiatric Association. DSM-5-TR — Diagnostic and Statistical Manual of Mental Disorders (2022)
- 8.Harvard Medical School. Harvard Health Publishing (2025)
- 9.Elsevier. Behaviour Research and Therapy (Elsevier) (2025)
Frequently Asked Questions

Written by
Valentina Lipskaya
Clinical Psychologist · Gestalt Therapist · CBT Specialist · ICF Certified Coach · MBA Professor
Panic Disorder, Anxiety, CBT & Gestalt Therapy
Valentina Lipskaya is a certified clinical psychologist and gestalt therapist specializing in panic disorders, anxiety, and neurological conditions. With over 15 years in psychology and 7 years of hands-on clinical practice, she has helped more than 750+ clients overcome panic, chronic anxiety, and psychosomatic conditions — without medication. Her work at Dzeny translates evidence-based therapeutic methods into practical, accessible guidance for everyday mental health.